Haemoglobin
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The haemoglobins are a group of chemically similar molecules found in many different organisms. Haemoglobin is a protein with a quaternary structure. The role of haemoglobin and red blood cells in the transport of oxygen.
Oxygen is transported around the body by haemoglobin (Hb), a globular protein with a quaternary structure found inside red blood cells. It consists of:
- Four polypeptide chains — two α chains and two β chains
- Each chain contains a haem group — a prosthetic group (a non-protein molecule permanently bound to the protein) with an iron ion (Fe²⁺) at its centre
- The Fe²⁺ ion binds oxygen, and each haem group can carry one O₂ molecule

Each Hb molecule can therefore bind up to four oxygen molecules, forming oxyhaemoglobin, a reversible reaction:
Haemoglobin + 4O₂ ⇌ Oxyhaemoglobin
Why iron deficiency causes anaemia
Each haem group requires an Fe²⁺ ion to bind oxygen. Without enough dietary iron, the body cannot produce sufficient haemoglobin, reducing the blood’s oxygen-carrying capacity. This is iron-deficiency anaemia. Symptoms include fatigue and breathlessness because tissues receive less oxygen for aerobic respiration.
How are red blood cells specifically adapted to maximise oxygen transport?
How are red blood cells specifically adapted to maximise oxygen transport?
- Biconcave disc shape — increases surface area and minimises the diffusion pathway to the centre of the cell
- No nucleus — maximises the volume available for haemoglobin
- No mitochondria — prevents oxygen being consumed in aerobic respiration during transport
Oxygen Dissociation Curve
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The loading, transport and unloading of oxygen in relation to the oxyhaemoglobin dissociation curve. The cooperative nature of oxygen binding to show that the change in shape of haemoglobin caused by binding of the first oxygens makes the binding of further oxygens easier.
To understand how haemoglobin loads and unloads oxygen, we first need to understand partial pressure.
Partial pressure of oxygen (pO₂) is a measure of oxygen concentration. The greater the oxygen concentration, the higher the partial pressure. The same applies to carbon dioxide (pCO₂).
- In the lungs, pO₂ is high → haemoglobin loads oxygen → oxyhaemoglobin forms
- In the tissues, pO₂ is low → oxyhaemoglobin unloads oxygen → haemoglobin is regenerated
The oxygen dissociation curve shows the percentage saturation of haemoglobin at any given pO₂.
The graph below shows three curves; click each one to explore what happens at low and high pO₂, and why the curve shifts position.
Cooperative Nature of Binding
If you look at the graph above, you can see it has a characteristic S-shape (sigmoid).
The S-shape arises because haemoglobin binds oxygen cooperatively:
- The first oxygen binds, changing the tertiary and quaternary structure of haemoglobin (start of curve, shallow)
- This conformational change makes the remaining binding sites more accessible
- The 2nd and 3rd oxygen molecules therefore bind more easily (steep rise in the middle of the curve)
- The 4th oxygen is slightly harder to bind as three of the four sites are already occupied (curve plateaus at the top)
Bohr Effect
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The effects of carbon dioxide concentration on the dissociation of oxyhaemoglobin (the Bohr effect).
In actively respiring tissues, CO₂ concentration is high. Carbon dioxide dissolves in the blood, forming carbonic acid, which lowers the pH. This decrease in pH causes a conformational change in haemoglobin which reduces its affinity for oxygen.
The result: the oxygen dissociation curve shifts to the right, so at any given pO₂, haemoglobin releases more oxygen.
Explain the advantage of the Bohr effect? (2 marks)
Explain the advantage of the Bohr effect? (2 marks)
- In actively respiring tissues, more CO₂ is produced → lower pH → haemoglobin has a reduced affinity for oxygen → more oxygen is released (1 mark)
- This increases the oxygen available for aerobic respiration, reducing reliance on anaerobic respiration and lactate production (1 mark)
Animal Adaptations to Environment
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
Many animals are adapted to their environment by possessing different types of haemoglobin with different oxygen transport properties.
Different animals have haemoglobin with different affinities for oxygen, adapted to their environment.
Animals living in low oxygen environments (e.g. high altitude, burrows) tend to have haemoglobin with a higher affinity for oxygen. Their dissociation curve shifts to the left, allowing them to load oxygen even at low pO₂.
Other instances of oxygen dissociation curve shifting to the left include:
- Foetal haemoglobin (HbF) also has a higher affinity for oxygen than adult haemoglobin (HbA), allowing the fetus to load oxygen from maternal blood across the placenta, where pO₂ is relatively low.
- Myoglobin, found in muscle cells, also has a higher affinity than haemoglobin. It acts as an oxygen store in muscles, only releasing oxygen when pO₂ is very low, such as during intense exercise.
Click the “High Altitude Animal” curve in the graph above to see a left-shifted curve in action.
Circulatory System
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The general pattern of blood circulation in a mammal. Names are required only of the coronary arteries and of the blood vessels entering and leaving the heart, lungs and kidneys.
Mammals have a double circulatory system: blood passes through the heart twice per circuit.
- Pulmonary circulation — right ventricle → lungs → left atrium
- Systemic circulation — left ventricle → body → right atrium

Why is a double circulatory system advantageous to humans?
Why is a double circulatory system advantageous to humans?
- In a single circulatory system, blood loses pressure as it passes through the lungs.
- A double circulatory system solves this: blood returns to the left ventricle after the lungs and is pumped at high pressure to the body.
- This maintains a high pressure in the systemic circulation, allowing oxygen and nutrients to be delivered to tissues quickly.
- It also keeps oxygenated and deoxygenated blood separate, increasing the efficiency of oxygen delivery.
Key named vessels you need to know:
| Location | Vessel entering | Vessel leaving |
|---|---|---|
| Heart | Vena cava (right side), Pulmonary vein (left side) | Aorta (left side), Pulmonary artery (right side) |
| Lungs | Pulmonary artery | Pulmonary vein |
| Kidneys | Renal artery | Renal vein |
Coronary arteries branch off the aorta and supply the cardiac muscle with oxygenated blood. Blockage causes a myocardial infarction (heart attack).
Blood Vessels
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The structure of arteries, arterioles and veins in relation to their function. The structure of capillaries and the importance of capillary beds as exchange surfaces.
Blood leaves the heart via the aorta and travels to the body’s tissues through five types of vessel, each adapted to its function:
Artery → Arteriole → Capillary → Venule → Vein

Arteries
Carry blood away from the heart at high pressure.
- Elastic tissue in the wall stretches and recoils to maintain pressure between heartbeats
- Smooth muscle (thick) withstands high blood pressure
- Smooth endothelium reduces friction
- Relatively narrow lumen maintains high blood pressure
Arterioles
Smaller branches of arteries that control blood distribution to capillaries. Blood flow must be regulated so that tissues receive blood according to their metabolic needs (e.g. during exercise, more blood is directed to skeletal muscles). Arterioles do this via:
- Vasoconstriction — smooth muscle contracts, narrowing the vessel and reducing blood flow to the capillaries
- Vasodilation — smooth muscle relaxes, widening the vessel and increasing blood flow to the capillaries
Veins
Return blood to the heart at low pressure.
- Large lumen — low resistance to blood flow
- Thin walls — only a small amount of elastic and muscular tissue, as blood is under low pressure
- Valves — to prevent backflow of blood
- Surrounding skeletal muscles squeeze the vein walls, pushing blood towards the heart

Capillaries
The site of gas and nutrient exchange between blood and tissues.
- One cell thick (single layer of endothelial cells) — very short diffusion pathway
- Very narrow lumen — slows blood flow, allowing more time for diffusion
- Extensive capillary beds — large surface area for exchange
Tissue Fluid
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The structure of capillaries and the importance of capillary beds as exchange surfaces. The formation of tissue fluid and its return to the circulatory system.
Cells do not receive oxygen and nutrients directly from capillaries. Instead, substances first leave the blood to form tissue fluid, a watery fluid that bathes all cells.
Tissue fluid contains small molecules (oxygen, glucose, amino acids, water) but not red blood cells, platelets, or large plasma proteins, as these are too large to leave capillary walls.
Formation of Tissue Fluid
- At the arteriole end of a capillary bed, the hydrostatic pressure inside the capillary is high.
- This forces fluid out through the capillary walls into the surrounding spaces, forming tissue fluid.
- Oxygen and nutrients can then diffuse from the tissue fluid into cells.

Reabsorption of Tissue Fluid
- As fluid is lost from the capillary, the plasma protein concentration inside increases (proteins cannot leave).
- This lowers the water potential of the blood relative to the tissue fluid.
- At the venule end, water moves back into the capillary by osmosis, along with dissolved waste products (CO₂, urea).

Summary
- Arteriole end: high hydrostatic pressure → fluid forced out of capillary
- Venule end: low water potential in blood → water drawn back in by osmosis
At the arteriole end, tissue fluid has a higher water potential than the blood. Why doesn't water simply move back into the capillary by osmosis here?
At the arteriole end, tissue fluid has a higher water potential than the blood. Why doesn't water simply move back into the capillary by osmosis here?
At the arteriole end, hydrostatic pressure inside the capillary is still very high. This hydrostatic pressure exceeds the osmotic gradient created by the plasma proteins, so the net movement of fluid is still outward, not inward.
It is only at the venule end that hydrostatic pressure has fallen (fluid has been lost from the capillary along the way). Here, the osmotic gradient, created by the plasma proteins that remain in the blood, becomes the dominant force, and water moves back in by osmosis.
Lymph
- Not all the tissue fluid is reabsorbed at the venule end.
- Excess fluid drains into the lymphatic system, which returns it to the circulatory system via the thoracic duct. Lymph is moved through the lymphatic vessels by the pressure of surrounding skeletal muscles.

Explore Tissue Fluid
- Small molecules (water, O₂, glucose) are carried in the blood inside capillaries alongside red blood cells and large plasma proteins.
- Use the simulation below to explore what happens at each end of the capillary bed, and predict what goes wrong in two abnormal conditions.
Oedema
Oedema is swelling caused by excess accumulation of tissue fluid. Two common causes:
High blood pressure
Increases hydrostatic pressure at the arteriole end, forcing more fluid out of capillaries than can be reabsorbed or drained by the lymphatic system.
Low plasma protein concentration
Raises the water potential of the blood, reducing the osmotic gradient at the venule end. Less fluid is reabsorbed, leading to accumulation in the tissues.
Heart
Heart Structure
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
The gross structure of the human heart.

The heart is made of cardiac muscle, which is myogenic. This means it can generate its own contractions without relying on nervous or hormonal input. It initiates its own contractions via the sinoatrial node (SAN) in the right atrium.
The heart has four chambers: right atrium, right ventricle, left atrium and left ventricle. Click each dropdown to explore the key features of the heart.
Atria (upper chambers)
Receive blood returning to the heart. Have thinner walls as they only pump blood a short distance into the ventricles below.
Ventricles (lower chambers)
Pump blood out of the heart. Have thicker, more muscular walls than the atria.
- The left ventricle is thicker than the right, as it must pump blood around the entire body (systemic circulation), while the right only pumps to the lungs (pulmonary circulation)
Septum
A muscular wall separating the left and right sides of the heart. Prevents oxygenated and deoxygenated blood from mixing.
Atrioventricular (AV) valves
Sit between the atria and ventricles (bicuspid on the left, tricuspid on the right). Prevent backflow of blood into the atria when the ventricles contract.
Semilunar (SL) valves
Sit at the exits of the ventricles into the pulmonary artery and aorta. Prevent backflow of blood into the ventricles after they contract.
Why is the left ventricle thicker than the right ventricle?
Why is the left ventricle thicker than the right ventricle?
The left ventricle must pump blood around the entire body (systemic circulation), a much longer distance at high pressure. The right ventricle only pumps blood to the lungs (pulmonary circulation), which are nearby and require far less pressure. The thicker muscular wall of the left ventricle generates the greater force needed for systemic circulation.
Coronary arteries branch off the aorta to supply the cardiac muscle itself with oxygenated blood. Blockage causes a myocardial infarction (heart attack).
Cardiac Cycle
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
Pressure and volume changes and associated valve movements during the cardiac cycle that maintain a unidirectional flow of blood.
The cardiac cycle describes the sequence of events in one heartbeat. Valves open and close in response to pressure differences: they open when pressure is higher on one side and close when it reverses, ensuring unidirectional blood flow.

Atrial Systole
- Atria walls contract → volume decreases, pressure increases
- Pressure in atria exceeds pressure in ventricles → AV valves open
- Blood is forced from atria into ventricles
- SL valves remain closed (arterial pressure exceeds ventricular pressure)
Ventricular Systole
- Ventricle walls contract → volume decreases, pressure increases
- Pressure in ventricles exceeds pressure in atria → AV valves close (prevents backflow)
- Pressure in ventricles exceeds pressure in aorta/pulmonary artery → SL valves open
- Blood is ejected into the aorta and pulmonary artery
Diastole
- All cardiac muscle relaxes → pressure in heart falls
- Pressure in aorta/pulmonary artery exceeds ventricular pressure → SL valves close (prevents backflow)
- Blood flows passively from veins into atria, then into ventricles
- AV valves open as atrial pressure exceeds ventricular pressure
Exam Questions
Give two structural features of an aorta wall and explain how they are related to the function of an aorta.
(2 marks)Hint
Name a tissue in the artery wall, then explain what it does during each heartbeat cycle. Think about what happens when blood surges through.
Mark Scheme
Any two of the following (1 mark each):
- (Smooth) muscle — absorbs/resists/withstands high blood pressure
- Elastic tissue — stretches and recoils, maintaining/smoothing blood pressure
- (Smooth) endothelium — reduces friction
- Protein coat — prevents the artery wall splitting / absorbs high blood pressure
Tips from examiner reports
- Muscles in artery walls don’t pump blood (a common misconception)
- Elastic tissue stretches when blood surges and recoils to smooth/maintain blood pressure; mention both stretch and recoil
- Vasoconstriction occurs in arterioles, not in the aorta
- The endothelium is smooth to reduce friction. Don’t confuse endothelium with epithelium
The dengue virus causes damage to capillaries so that blood proteins move out of the capillaries into the tissue fluid.
Explain how damage to capillaries would affect the return of tissue fluid into the capillaries.
(2 marks)Hint
What happens when protein leaks out of capillaries? How does this affect water potential in the blood and the direction of water movement?
Mark Scheme
- Increases water potential of blood/capillary OR decreases water potential of tissue fluid (1 mark)
- So less water returns to blood/capillaries by osmosis OR more water leaves blood/capillaries by osmosis (1 mark)
Comments from mark scheme
- Accept Ψ for water potential
- Accept “reduces water potential gradient”
- Accept “no” for less
Tips from examiner reports
- It’s water that moves by osmosis, not tissue fluid; be precise with terminology
- If protein leaks out of capillaries, water potential of the blood increases (not decreases). Proteins lower water potential, so losing them raises it
- State clearly where the water potential changes and the direction of water movement
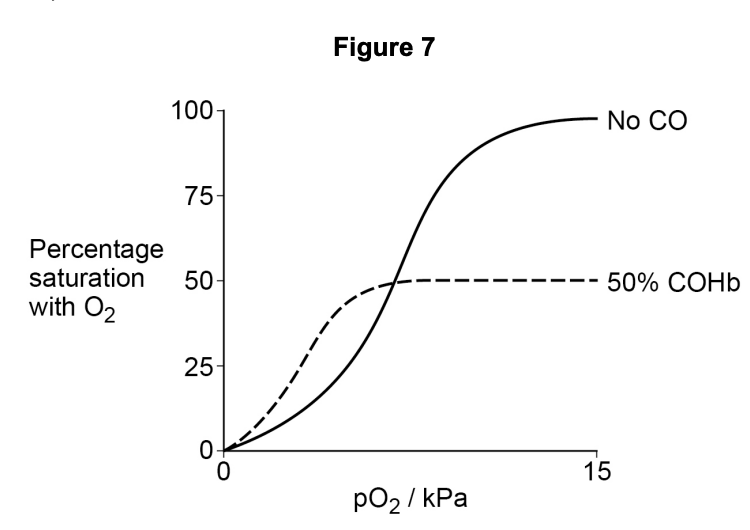
Carbon monoxide (CO) is released during incomplete combustion of fossil fuels. Figure 7 shows the dissociation curve for oxyhaemoglobin when:
- not exposed to CO
- exposed to CO such that 50% of the oxygen binding sites are occupied by CO (50% COHb)
Using Figure 7, what can you conclude about how exposure to CO affects the loading and unloading of oxygen by haemoglobin? Explain your answer.
Hint
Apply knowledge specifically to carboxyhaemoglobin (COHb). How does CO affect oxygen loading AND unloading? Don’t just recall general dissociation curve knowledge; use the graph.
Mark Scheme
- Less oxygen loaded at high pO₂ (compared with no CO) OR maximum Hb saturation is 50% (1 mark)
- At low pO₂, Hb has higher affinity for oxygen (1 mark)
- Hb has more oxygen at low pO₂ OR Hb unloads less oxygen at low pO₂ (1 mark)
Comments from mark scheme
- Ignore references to “binding sites occupied by CO”
- Accept “in lungs” for “high pO₂”
- Accept “levels off” or “plateau at 50%” for maximum saturation
- Accept “in respiring cells/tissues” for “low pO₂”
- Accept “less readily” for less
Tips from examiner reports
- Apply oxygen dissociation curve knowledge to the specific context; don’t just describe a normal curve
- Carbon monoxide binds to haemoglobin and prevents oxygen loading; don’t say COHb “loads more readily”
- The Bohr shift and pH changes are not relevant to carbon monoxide poisoning
Comments from mark scheme